EMBRYOLOGY
AND PATHOPHYSIOLOGY
The class IV
malformation (Bicornuate uterus) is caused by partial
non-fusion of the upper part of the mullerian ducts.
This results in a central myometrium that may extend to the level of the
internal cervical os (bicornuate
unicollis) or external os (bicornuat bicollis), with a
fundal cleft.1cm deep.3–6The
horns of the bicornuate uteri are not as fully
developed and are smaller than those in the didelphys
uteri.
CLINICAL
FEATURES
Patients with bicornuate uterus are usually asymptomatic but can present
with symptoms like menorrhagia and dysmenorrhea which are non-specific symptoms
and also a history of recurrent miscarriage, preterm deliveries and persistent
abnormal lies and presentation in pregnancy.2–4 The diagnosis is
usually made as an incidental finding during evaluation for infertility and
patients with recurrent miscarriage.2–4,7
INVESTIGATIONS
It is
important to differentiate a bicornuate from a septate uterus. Hysterosalpingogram
(HSG) alone cannot differentiate these entities, because this imaging approach
cannot evaluate the external contour of the uterus.8 While laparoscopy
was used primarily for this purpose in the past, modern imaging techniques
including 3D ultrasonography and MRI can adequately differentiate these two
entities. Imaging criteria to differentiate septate
and bicornuate uteri have been developed. A septate uterus has a flat or convex fundus or a fundal
indentation 60°.3,8 On MRI, a septate
uterus will fail to show an intervening myometrium between the T2- hypointense septum that separates the endometrial cavities
[80, 81]. In contrast, a bicornuate uterus will show
two T2-hyperintense endometrial cavities, each with a junctional
zone and myometrial band of intermediate signal
intensity.
Endoscopic
procedures like laparoscopy and hysteroscopy are diagnostic and therapeutic.
MANAGEMENT
Most cases
of Bicornuate uterus may not need any treatment
unless they are associated with infertility, recurrent pregnancy loss or
Uterine pathologies like fibroids.6,8
Conventional
transabdominal metroplasty
has been shown to significantly improve the pregnancy outcome in patients with bicornuate uterus.2,8 Laparoscopic approach is also technically challenging but
offers the general positive benefits of endoscopic surgeries. Thus, the
most common surgical treatment options for bicornuate
uterus may include the Strassman metroplasty
and cervical cerclage. The surgery entails removing the abnormal tissue that
separates the cornua of the uterus, then using
several layers of stitches to create a normal shape and single uterine cavity.
The pregnancy rate following metroplasty has been
seen in up to 90% of cases.4
CASE REPORT
A 35 year old nulliparous woman who presented to
the gynaecological clinic with complaints of
recurrent lower abdominal pains, dysmenorrhea and abdominal mass of 3 years
duration. There was no menorrhagia,
urinary or pressure symptoms from the mass.
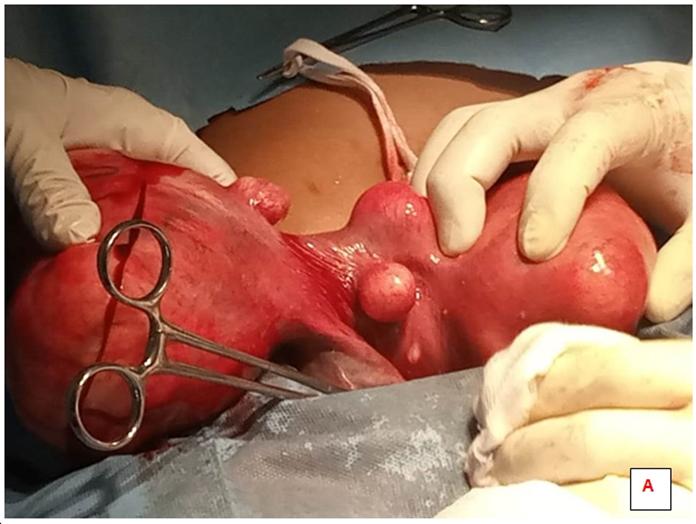
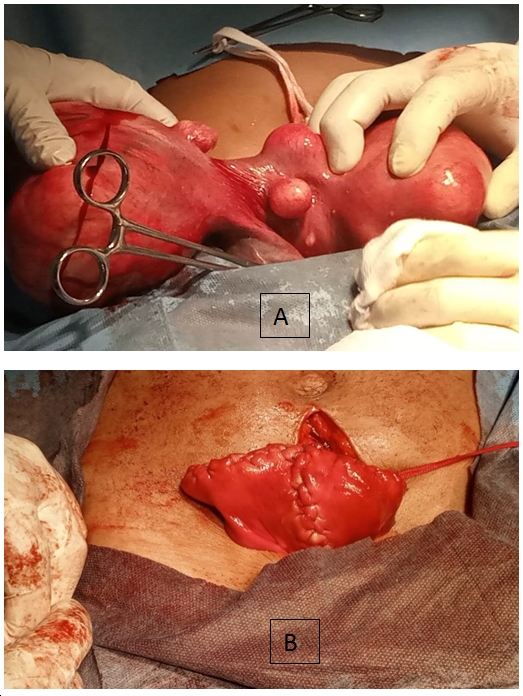
Abdominal examination revealed a 22 week sized abdomeninopelvic mass. She was evaluated for symptomatic
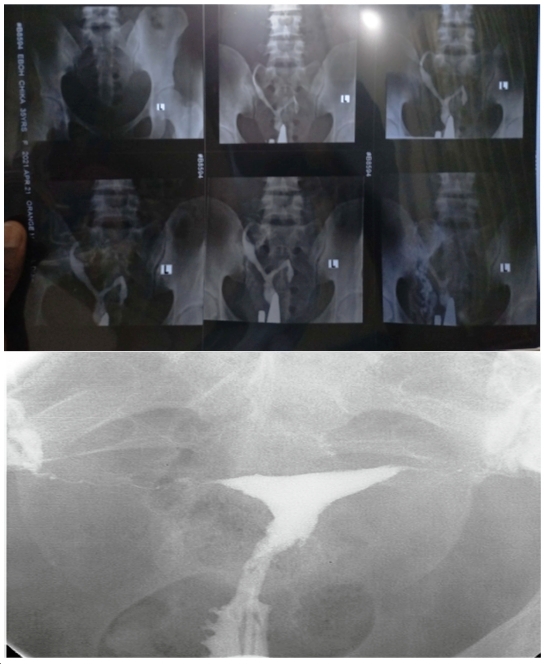
uterine fibroids. Incidentally the hysterosalpingography
revealed a congenitally malformed uterus, suggested to be bicornuate
uterus. She was further assessed using a diagnostic hysteroscopy which showed
the obvious septation with the two cavities. An
intravenous urography ruled out a pathology of the
urinary system. These are shown in figure 2.
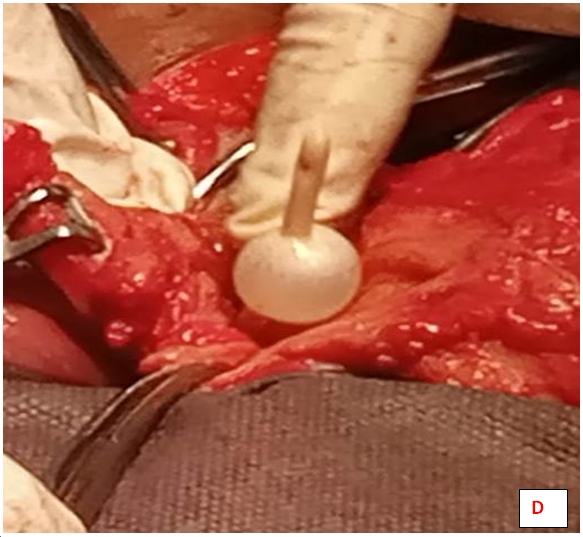
The
post-operative period was uneventful and an intra-uterine foleys
catheter was inserted to keep the cavity patent. It was removed after 10 days.
The patient was given conjugated estrogen for 21 days and medroxyprogesterone
for last 10 days for 6 months.
DISCUSSION
Uterine bicornis was an asymptomatic incidental finding in course
of radiographic studies of the uterus of this patient. Complimentary
hysteroscopy review confirmed the earlier noted findings. There was also no
tubal patency on HSG, which maybe as a result of the huge fibroids on the horns
of the uterus. This is the usual pattern of arriving at a diagnosis for most
cases of Bicornaute uterus and other congenital
anomalies of the uterus.9–12
There are
very few cases of fibroids co-existing with Mullerian
anomalies reported in literature and thus the diagnosis is not often made
because of the low incidence.13
Metroplastic surgery
was described by Strassman in 1952 for class III, IV
and V anomalies, and it was subsequently modified and simplified by Jones in
1953 (wedge excision of the septum) and Tompkins in 1962 (incision of the
septum).4,14
Open
conventional metroplasty and laproscopy
for the treatment of Bicornuate uterus are both safe
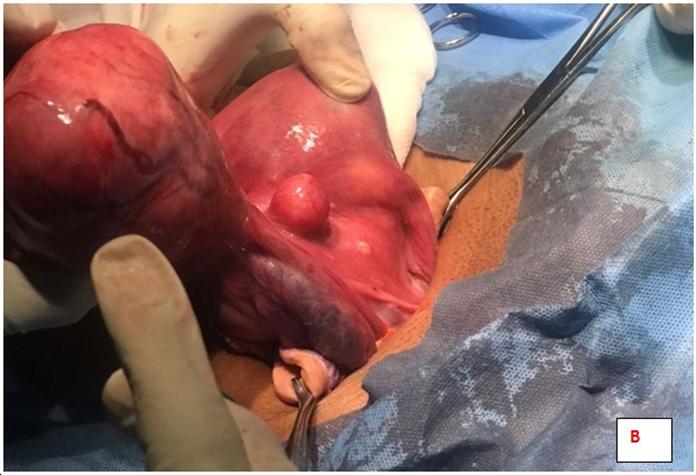
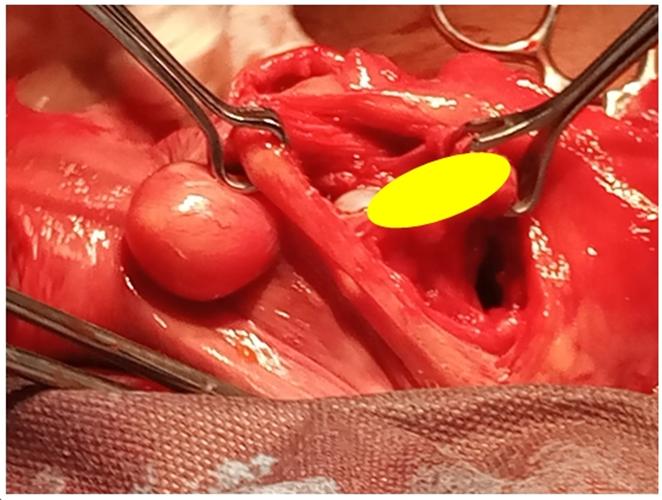
and viable options.8 The patient had an
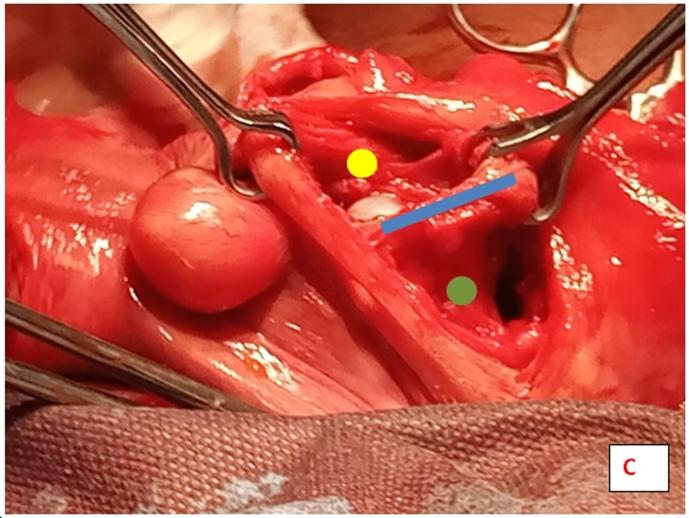
abdominal modified strassman’s metroplasty
that involved excision of the septum. This procedure has been widely practiced
in the few symptomatic cases of Bicornuate ueterus.4,8 Inra-operatively,
in the hands of a skilled surgeon adequate care may be taken to ensure that the
myometrial edges are not sutured under tension, as it
is prone to hematoma formation.
In this
patient laparoscopy was indicated as an option, but considering the multiple
uterine fibroids, its size and unavailability of the facilities and experience,
an open abdominal procedure was considered.
Post-operative
hysterosalpingography studies confirmed a single
cavity and patent tubes. Pregnancy has been widely reported following metroplasty, although there is increased risk of placenta previa, morbidly adherent placenta and uterine rupture.15–18
Considering the age
of the patient, even though nulliparous, pregnancy outcome as recorded in
literature holds a good prognosis for the patient.19
CONCLUSION
The correction of uterine anomalies is recommended in
patients who show symptoms. Surgical metroplasy has
been shown to be an effective method of treatment of the symptomatic patients
and also offers improvement in fertility and pregnancy outcome.
The use of laparoscopic approach to myomectomy and metroplasty is gaining grounds worldwide and Africa need to
rise up to the occasion in order to offer patients the benefits of these
advancements in clinical practice.
REFERENCES
1. Saravelos SH, Cocksedge KA,
Li TC. Prevalence and diagnosis of congenital uterine anomalies in women with
reproductive failure: A critical appraisal. Hum Reprod Update.
2008;14(5):415–29.
2. Subburaj L, Rajkumar K. Laparoscopic
metroplasty for bicornuate uterus – A case report. Indian J Obstet Gynecol Res.
2021;8(2):279–81.
3. Chandler TM, Machan LS, Cooperberg PL,
Harris AC, Chang SD. Müllerian duct anomalies: From diagnosis to intervention.
Br J Radiol. 2009;82(984):1034–42.
4. Passos I de MP e., Britto RL. Diagnosis
and treatment of müllerian malformations. Taiwan J Obstet Gynecol.
2020;59(2):183–8.
5. Ribeiro SC, Tormena RA, Peterson TV,
Gonzáles M de O, Serrano PG, de Almeida JAM, et al. Müllerian duct anomalies:
Review of current management. Sao Paulo Med J. 2009;127(2):92–6.
6. Yadav A, Prateek S, Chawla L, Sharma S,
Choudhary D. Bicornuate Uterus with Unilateral Fibroid - Surgical Procedure or
LNG-IUS – A Conservative Approach in a Patient Who Opted LNG as Contraception.
J Evol Med Dent Sci. 2020;9(39):2924–6.
7. Nwankwo NC, Maduforo CO. Mullerian duct
anomaly in a Nigerian woman with recurrent pregnancy loss. Niger J Clin Pract.
2011;14(1):109–11.
8. Attaran M. Surgical Techniques for
Management of Anomalies of the Müllerian Ducts. In: Clinical Reproductive
Medicine and Surgery. 2017. p. 461–85.
9. Hg I, Sb M, Ar H, Ua U. Bicornuate Uterus
Presenting with Recurrent Pregnancy Loss ; the Role of
Hysterosalpingography in the Diagnosis : A Report of Two Cases.
2020;10(December):270–3.
10. Ludwin A, Ludwin I, Banas T, Knafel A,
Miedzyblocki M. Diagnostic accuracy of sonohysterography ,
hysterosalpingography and diagnostic hysteroscopy in diagnosis of arcuate ,
septate and bicornuate uterus. 2011;37(3):178–86.
11. Article O. Comparative Prospective Study of
Hysterosalpingography and Hysteroscopy in Infertile Women. 2017;
12. Tsonis O. Sonographic and Hysteroscopic
Assessment of Uterine Congenital Journal of Medical - Clinical Research &
Reviews Sonographic and Hysteroscopic Assessment of Uterine Congenital
Malformations : A Retrospective Study. 2021;(April):1–5.
13. Bafna B, Bafna A, Bafna A. Uterus bicornis
unicollis with multiple lieomyomas. Int J Reprod Contraception, Obstet Gynecol.
2016;5(11):4088–90.
14. Matsaseng T, Kruger TF. Laparoscopic
Strassman’s metroplasty for bicornuate uterus -is it relevant? S Afr J Obstet
Gynaecol. 2012;18(3):85–7.
15. Zhang C, Wang X, Jiang H, Hou L, Zou L.
Placenta percreta after Strassman metroplasty of complete bicornuate uterus: a
case report. BMC Pregnancy Childbirth. 2021;21(1):1–5.
16. Zhou QY, Saravelos S, Huang XW, Ma N, Li T,
Xia EL. Laparoscopic metroplasty for bicorporeal uterus: surgical techniques
and outcomes. Chin Med J (Engl). 2020;134(9):1107–9.
17. Ono S, Yonezawa M, Watanabe K, Abe T, Mine
K, Kuwabara Y, et al. Retrospective cohort study of the risk factors for
secondary infertility following hysteroscopic metroplasty of the uterine septum
in women with recurrent pregnancy loss. Reprod Med Biol. 2018;17(1):77–81.
18. Gulavi E, Kyende Mutiso S, Mariara Muriuki
C, Mukaindo Mwaniki A. Successful Pregnancy Outcome after Open Strassman
Metroplasty for Bicornuate Uterus. Case Rep Obstet Gynecol. 2018;2018:1–4.
19. Wang X, Hou H, Yu Q. Fertility and
pregnancy outcomes following hysteroscopic metroplasty of different sized
uterine septa: A retrospective cohort study protocol. Med (United States).
2019;98(30).