INTRODUCTION
Malrotation with associated
duodenal obstruction is a commoner presentation of infants compared to adults.[1,2] A prevalence of 0.17 percent was observed amongst
adults in a study carried out by Perez and Pickhardt.[3]
The gut undergoes a
270o counterclockwise rotation around the superior mesenteric
vessels during physiologic herniation and return with fixation of the duodenojejunal loop to the left of the midline and the
cecum in the right lower quadrant. Any variation in this rotation and fixation
of the gut during development results in intestinal malrotation,
which could be intestinal nonrotation or incomplete rotation.[4,5]
Malrotation can present as
either an acute or chronic process viz – Acute midgut volvulus, Chronic midgut
volvulus, Acute duodenal obstruction, Chronic duodenal obstruction as well as
Internal herniation. The typical age at diagnosis of Chronic
duodenal obstruction ranges from infancy to preschool-age. The most common
symptom is vomiting, which is usually bilious and intermittent abdominal pain
(frequently diagnosed as colic). The patients may also have failure to thrive.[4]
Upper gastrointestinal
contrast study is useful to confirm the diagnosis and Ladd procedure remains
the cornerstone of treatment.[2,4,6]
CASE REPORT:
A 23-year-old female undergraduate who has
been experiencing recurrent upper abdominal pain and vomiting over the past 13 years presented to the general
surgery clinic. The pain was majorly in the epigastric
region, sharp and colicky, aggravated with meals, non-radiating, non-periodic,
no relieving factors, no dyspepsia. Vomiting occurred 2 – 4 times a day mostly
following feeds. It contained recently ingested food, about 100 – 300ml per
episode, sometimes bilious but non projectile and no haematemesis.
There was associated poor weight gain. Physical examination revealed a young
lady who was underweight with epigastric fulness and the rest of the abdomen scaphoid. There was
occasional visible peristalsis in the upper abdomen.
Barium meal done showed narrowing of the
post bulbar portion of the 2nd part of the duodenum in the prone position only.
While abdominal ultrasound scan revealed an anomalous vessel in the retroperitoneum around the duodenum and pancreas
compressing the duodenum. A diagnosis of duodenal obstruction due to malrotation was considered and patient counselled
for laparotomy.
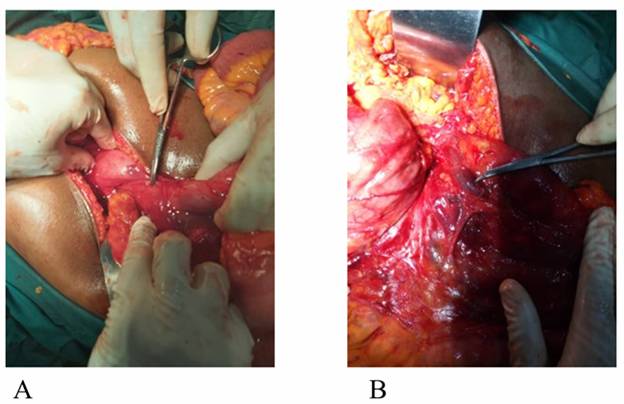
Findings during surgery were:
- Freely mobile cecum located in the left
paracolic gutter with an uninflamed
appendix measuring about 10cm, figure 1.
- Collapsed small intestine disposed to
the right paracolic area and abnormally located duodenojejunal junction.
- Dilated duodenum, up to the 3rd part,
with anomalous vessels crossing the anterior aspect of that part,
compressing adherently on the duodenum with a kink, figures 2 and 3.
- External Ladd's band holding the
duodenum to the retroperitoneum.
- Other organs appeared normal and in
their usual anatomic position
Release
of Ladd’s bands and abnormal vessels causing duodenal obstruction was done; as
well as appendectomy. The bowel was then placed in the position of
non-rotation.
The patient had a good recovery and was
discharged on post operative day 6. She maintained a
progressive improvement with weight gain on subsequent follow-up visits.
DISCUSSION:
Malrotation cases sometimes are
seen in adult patients, albeit the vast majority are observed in the first
month of life.[1-3] Our index patient appeared to have
been asymptomatic in childhood but started developing symptoms from early
adolescence which progressed to adulthood. As demonstrated by this case, adult
patients commonly present with vomiting and recurrent abdominal pain (often
postprandial) as well as weight loss. [7,8] These
symptoms are probably due to chronic partial upper intestinal obstruction. [9,10]
Other presentations include early satiety with bloating, dyspepsia with peptic
or duodenal ulcer disease, diarrhoea, malabsorption, peritonitis with septic shock, etc. [8] This
condition might manifest as chronic nonspecific symptoms in some adults, making
it difficult to establish a diagnosis. [11] Some of such patients become labelled with functional or psychiatric disorders and never
get surgical referral. [12]
It is therefore of
utmost importance to have a high index of suspicion and to endeavour
to arrive at a specific diagnosis when adults present with nonspecific
abdominal discomfort and chronic intermittent abdominal pain. Routine imaging
studies with contrast has been shown to be very valuable in making diagnosis. [13] However, Sala et
al in their study describe computed tomography scan as the method of choice for
the diagnosis of malrotations [14]. Upper
gastrointestinal barium studies and abdominal ultrasound scan were done for the
index patient; and the combination provided a good pre-operative evaluation of
the condition.
Ladd's procedure,
first described in 1936, remains the mainstay of treatment regardless of age at
presentation.[6] The procedure involves mobilization
of the duodenum and right colon, division of coloduodenal
adhesions (Ladd's bands) which may be sometimes near the superior mesentery,
broadening of the mesenteric base to prevent volvulus but if volvulus is
present counterclockwise reduction of the volvulus is done before widening of
the mesenteric base to prevent repeated volvulus. Also, prophylactic
appendectomy is done because of potential difficulty in diagnosing appendicitis
in the future, since the appendix will now be in a location far from the normal
anatomic location after the bowel is placed in the position of non-rotation. [15].
To be abreast with the Ladd's procedure, it is very
important that surgeons operating on adults get thorough knowledge of
intestinal embryology and its anatomic variations. In the index case, the
assistance of a paediatric surgeon was required at
the surgery.
For the index case,
Ladd’s bands were released and the abnormal vessels crossing anteriorly to the
duodenum were separated from it. The mesentery was then broadened and
prophylactic appendectomy done; there was no volvulus in this case. The bowel
was eventually placed in the position of non-rotation as described by Ladd.
In conclusion, this case highlights the need for a high index of suspicion
of malrotation with chronic duodenal obstruction in
adults presenting with recurrent abdominal pain and vomiting associated with
weight loss. Also, there is the need for surgeons operating on adults to be
very acquainted with the surgical procedure of treatment of such cases.
REFERENCES:
1.
O.F. Emanuwa, A.A. Ayantunde,
T.W. Davies. Midgut malrotation
first presenting as acute bowel obstruction in adulthood: a case report and
literature review.World J. Emerg.
Surg., 6 (1) (2011), p. 22
2.
Wang CA, Welch CE.
Anomalies of intestinal rotation in adolescents and adults. Surgery. 1963;
54:839–955.
3.
Perez AA, Pickhardt PJ. Intestinal malrotation in adults: prevalence and findings based on CT colonography. Abdom Radiol (NY) 2021; 46:3002.
4.
Dassinger MS, Smith SD. Disorders of Intestinal
Rotation and Fixation. In: Coran AG, Adzick NS, Krummel TM, Laberge J-M, Shamberger RC and Caldamone AA (eds.). Paedatric Surgery. 7th ed. Saunders, an imprint of Elsevier
Inc, Philadelphia. 2012, pp. 1111-1125.
5.
Dott NM. Anomalies of intestinal rotation: Their
embryology and surgical aspects: With report of five cases. Br J Surg. 1923;
11:251–286.
6.
Ladd WE. Congenital
Obstruction of the Duodenum in Children. N Engl J
Med. 1932. 206:277-80.
7.
Yanez R, Spitz L. Intestinal malrotation
presenting outside the neonatal period. Arch Dis Child. 1986; 61:682–685.
8.
Spigland N, Brandt ML, Yazbeck
S. Malrotation presenting beyond the neonatal period.
J Pediatr Surg. 1990; 25:1139–1142.
9.
A.K. Wanjari, A.J. Deshmukh, P.S. Tayde, Y. Lonkar. Midgut malrotation with chronic
abdominal pain. North Am. J. Med. Sci., 4 (4) (2012), p. 196
10.
E.A. Ameh, P.T. Nmadu. Intestinal volvulus: aetiology,
morbidity, and mortality in Nigerian children. Pediatr.
Surg. Int., 16 (1–2) (2000), pp. 50-52
11.
Dilley AV, Pereira J, Shi EC, et al. The
radiologist says malrotation: does the surgeon
operate? Pediatr Surg Int.
2000; 16:45–49.
12.
Gamblin
TC, Stephens RE Jr, Johnson RK, Rothwell
M. Adult malrotation: a case report and review of the
literature. Curr Surg. 2003; 60:517–520.
13.
C. Duran, E. Ozturk,
S. Uraz, A. Kocakusak, H. Mutlu, Killi, R.
Midgut volvulus: value of multidetector
computed tomography in diagnosis. Turk. J. Gastroenterol.,
19 (3) (2008), pp. 189-192
14.
Sala
MAS, Ligabô AN, de Arruda
MCC, Indiani JMC, Nacif MS.
Intestinal malrotation associated with duodenal
obstruction secondary to Ladd's bands. Radiol Bras.
2016 Jul-Aug; 49(4): 271–272.
15.
Gamblin
TC, Stephens RE Jr, Johnson RK, et al. Adult malrotation: a case report and review of the literature. Curr Surg. 2003; 60:517–520.