INTRODUCTION
Maternal
mortality is of global concern in low income nations in the world especially in
sub Saharan Africa, particularly Nigeria. Maternal mortality ratio is 814 per 100,000 live births in
Nigeria, one of the highest in the world (Bill Gate, 2018). Major causes of
maternal mortality include: hemorrhage, sepsis, and obstructed labor,
complications of induced abortion and hypertensive disease of pregnancy. These
preventable causes of maternal death are propagated some socio-economic and
cultural factors (Hogan,2010); most of these women did
not receive antenatal care, reported late in hospital when they developed
complications or were attended to at delivery by unqualified personnel (CIA
World Factbook, 2015). According to Nigerian Demographic and Health
Survey, only thirty percent of Nigerian women deliver in health
institutions. Majority of them had their
antenatal care and delivery Faith-based centers ((Sloan RP, 2006)
In this study the frame work is based
on the theory of Functionalism developed by Emile Durkheim and updated Bn8
(2021) examines religion from a viewpoint of societal needs; that as an
integral part of the sacred world, religion serves as a means of controlling human
actions and behavior
Malinowski in their support for Durkheim said
that religion being part of the cultural system provides general rule for human
behavior and criteria for the evaluation of human conduct updated in Sociology guide.com (2021).
There are countless numbers of faith-based health institutions providing
healthcare services in both urban and rural areas in this country but little
has been accomplished in the use of religion to boost utilization of maternal healthcare
services particularly in addressing maternal mortality. Worst still, the
doctrines and teachings of some religious institutions hinder reproductive
healthcare utilization with fatal consequences (Udoma,
Ekanen, 2008).
The myth “I must deliver like the
Hebrew women; Caesarian section is not my portion” (Exodus 1 :15-21); is a
misconception that has brought many women ignorantly to an early grave as
stated by prophet Hosea in the Holy Bible “My people perish for lack of
knowledge.” (Hosea 4:6).
Religion
Religion
has been defined as an organized system of belief, practices and symbols
designed to facilitate closeness to God as well as providing foundation and
support that enable people have a sense of well-being and wholeness ((CIA World
Factbook, 2015).) It serves as an outstanding social
institution that shapes individuals and community, heal behavior through its
influence on lifestyle, world view and motivation (,(CIA
World Factbook, 2015).). Some of the ways religion influences health include:
1.
Health behavior, achieved by discouraging some harmful habits such
as the abuse of alcoholic beverages, smoking, this protects and promotes
healthy lifestyle.
2. Social Support: done by creating a network of social
contacts with co-religionists (members of same Church/ mosque/organization)
that can help in times of need.
3. Stabilizes
psychological states: a
better mental health, more positive mental status, more optimism which in turn can eventually lead to a
better physical state, reducing stress.
4. Strong belief in the supernatural law and the Supreme Being (God) that governs all
things ((CIA World Factbook, 2015).).
Maternal
Mortality.
Maternal mortality is defined as “death
of a woman while pregnant or within 42 days of termination of pregnancy,
irrespective of the duration and site of the pregnancy from any cause related
to or aggravated by pregnancy or its management” (Hogan,2010
)
There are three delay models by which
to understand religion as a social constraint that affects maternal outcome:
1.
Delay in recognizing danger signs and
deciding to seek care.
2.
Delay in reaching an appropriate source
of care.
3.
Delay in obtaining adequate and
appropriate treatment, (Ugwu and de Kok ,2015).
Some
religious sects do not approve use of modern drugs and medical sundries: shows
lack of faith in God. b) That everything that happens to a person originates from
the spiritual realm including complications in pregnancy ,
thus they force the women to confess their sins instead of taking them to
hospital ( Maguranyanga ,2011). Child spacing in terms of limiting fertility
is the first gate to avoiding maternal mortality but high fertility is
doctrinally supported and contraception is believed to be contrary to God's
commandment saying, “Go ye, multiply, be fruitful and replenish the earth.”( Genesis 1:28 KJV 2014). The Jehovah Witness discourage
blood transfusion
e)
Several other Christian groups advocate seeking spiritual counsel and faith
healing should the use of medicine health problems are caused by the influence
of wrath of God as punishment for sin and demon possession (Tanyi
RA,2006).
f) Some
religious sectors see nothing to fear in a woman’s bleeding (Hebrew 9:22 KJV
2014.); that giving birth should involve blood loss without which there cannot
be life.
In prayer
houses deliveries are often undertaken by unskilled attendants in a probably
unhygienic environment and complications at such centers are commonly blamed on
the parturient, accusing her of witchcraft or unfaithfulness to her husband(( Maguranyanga ,2011).).Even some booked pregnant women
attending Antenatal Care (ANC) in hospitals still end up having child
birth/delivering in prayer houses/mission homes (Maguranyanga ,2011).
RESEARCH
METHODOLOGY
Research
Design
This
study was a hospital based 5 years retrospective survey.
Population and Sample
This
consisted of all deliveries/childbirths, maternal deaths that occurred in Zonal
Hospital Bori within the five year period of January
2013 to December, 2017. Referrals from
mission homes, church maternities, traditional birth attendants and health
centers to the Hospital within the 5 years study period were also included.
Simple serial recording of the data
collected from the birth register of the maternity and the patient’s hospital
folders from the medical records department.
Instruments
for the data collection were:
1. Birth register from the maternity
departments.
2. The patients’ folders from the Medical Record
Department.
3.
Interview
of selected stakeholders
Approval
was first obtained for the collection of data from the Rivers State Health
Research Committee and the Medical Director of Zonal Hospital Bori respectively.
Epidemiological data was collected from the birth register of the
maternity and from the patients’ folders at the Medical Records Unit of the
Hospital. All cases referred from mission homes, traditional birth attendants
and other health centers were documented.
Method
of Data Analysis
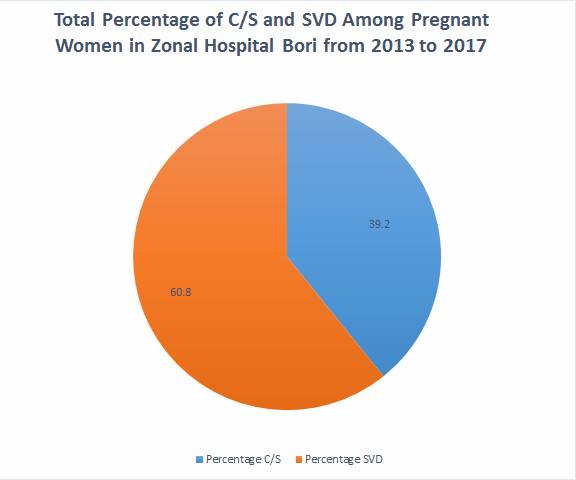
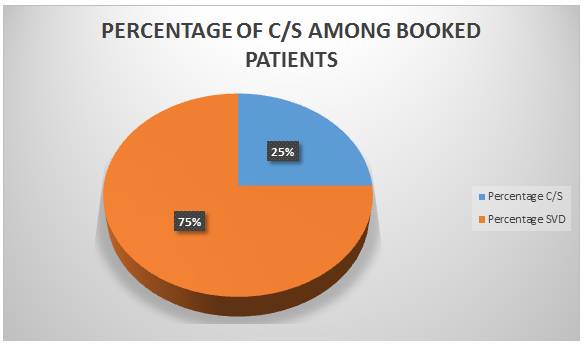
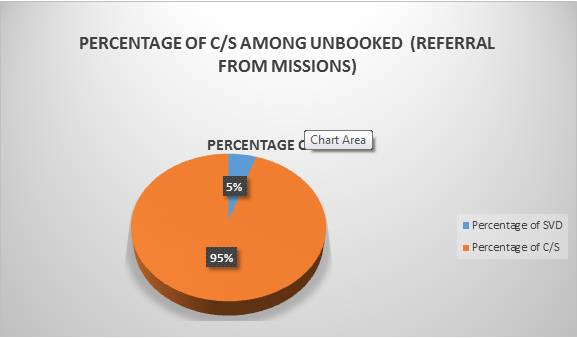
Quantitative data obtained from serial
recording of the number of childbirths, maternal deaths, number of women that
had normal delivery, assisted vaginal delivery and caesarian section were analysed along with the data from all the referrals using
tables and pie chart.
Qualitative data were obtained from
Interviews of some stakeholders.
The stakeholders interviewed included:
Pregnant women attending Ante-natal care (ANC) at the Hospital, post operative
mothers who were referred for prolonged obstructed labour
and other complications of pregnancy
from alternative health care providers. Church leaders
from churches that have maternity homes for their doctrine and teaching
regarding child birth.
The alternative care providers
themselves as regards the care of the parturient at their mission homes church
maternities:
The
interviews provided
views of the pregnant
women as regards abdominal delivery (C/S). It also explored reasons behind
patronage of alternative health care providers, how religious
teachings/doctrines and some socio-cultural values affect the health seeking
behavior of the parturient women relating to CS (Ugwuandde Kok 2015)
It was surprising to note from the
respondents that some of the pregnant women who were duly attending antenatal
care at the hospital preferred to deliver at prayer houses, especially those
who were counseled for operative delivery, affirming “Abdominal delivery is not
my portion, I must deliver like the Hebrew
women.” This notion is usually worsened
by “prophesies” and “visions” from some of their pastors and fellow believers
who would specifically warn them against hospital delivery and going through
surgery. It was also observed that most of the un-booked mothers coming from
prayer houses, mission homes, and traditional birth attendant homes usually
arrived at the hospital very late with obstetric complications such as
postpartum hemorrhage, obstructed labor, and sepsis. Upon brief clerking on
arrival at the hospital, the women saw the pregnancy complications as an
“attack,” a spiritual manipulation. When
asked why they preferred spiritual houses, most said their pregnancies were
under “attack” from their enemies, they therefore needed a place where prayers
would be offered for their safe delivery.
On why the late arrival at the hospital, some said the pastor in charge
of the mission home was not immediately available to pray for them and release
them from the home. In some cases, referrals were made very late, which means
the birth attendants at the prayer houses, churches and mission homes were not
skilled enough to detect the obstetric complications early. It was however observed in some cases that
referrals were made late at night and fear of insecurity, and logistics
arrangement for transportation and money especially if the husband was not
available, made them arrive the following morning when it was too late for any
meaningful intervention.
The Setting
Zonal Hospital Bori
Zonal
Hospital Bori is a secondary healthcare facility with
a capacity of 79 beds owned by the Rivers State Government. The hospital is affiliated to Rivers State
University Teaching Hospital and University of Port Harcourt Teaching Hospital
as a center for rural posting for training of residents in Family Medicine,
Surgery, Anaesthesia, Obstetrics and Gynecology.
The
Obstetrics and Gynecology Unit of the Zonal Hospital Bori
runs antenatal clinic three times a week..
There is a very functional maternity
unity which takes an average of one hundred deliveries monthly. Trained, skilled and experienced midwives
used to take normal deliveries, while complications in pregnancy and labour are usually handled by the emergency obstetric
team. The maternity unit receives
referrals from the rural communities: from the traditional birth attendants
(TBAs), mission homes, church maternities, primary health centers and private
hospitals. The catchment area of the hospital includes the various rural
communities of Ogoni with the neighbouring
Local Government Areas of Opobo-Nkoro and Andoni.W
Ogonias a People
Ogoni has four local government areas
namely, Khana, Gokana, Tai
and Eleme, with a total population of about 1,000,000
people. They inhabit the coastal plains
and terrains of the Niger Delta in Rivers State, South-South Nigeria and live
on an area of 650 mg kilometers resulting in a very high population density
(Niger Delta Liberation Project. ,2005). Farming and fishing are their main
occupation, though a few pursue their career in different works of life. The
gross environmental pollution over the years affecting aquatic life and
vegetation rendered the sea and the farmland unproductive for fishing and
farming respectively. The people are therefore generally poor. Poverty made them more religious and hence
their patronage of alternative health care providers,
especially the pregnant women.
DISCUSSION
Maternal Mortality in Bori, Ogoni
The religious factors associated
with the high Maternal Mortality in BORI
Bori people see pregnancy as a message from
God and the pregnant woman as a messenger.
It therefore follows that any complication in the pregnancy is usually
tied to spiritual forces countering the divine purpose of God in the life of
the messenger ( the pregnant woman); sad events such
as maternal deaths or death of the baby during childbirth are usually
attributed to the anger of ancestral spirits who are either demanding for
unpaid dowry on the woman or a penalty for an offence committed by the woman
making them drift to prayer meetings, mission homes and church maternities.
The firm belief that childbirth
should be through vaginal delivery and must not be through operation (C.S.)
The effect of false ‘prophecies
and visions’ concerning the pregnancy and child birth.
Participants’ views on the
possible reasons why a woman may need a CS:
Extracts from pregnant women attending Antenatal Care(ANC) at
Zonal Hospital Bori.
P1 ”…. pregnancy is a message
from God; God who put the baby there
will know how to remove it at the right time since we are all messengers , I
don’t have any fear”
P2 ” …. asa woman I must deliver like the Hebrew women, God
will not allow my enemies to laugh at me;
operation( c/s) is not my portion”
Extracts from
patients referred for prolonged obstructed labour (post operative).
P3……” it will not
be well with whoever has tied my womb, for me to have this operation. A man told me earlier in the pregnancy that
he would see whether I would deliver through my mouth…..”
There
were three cases of very big babies, 4.5kg which caused prolonged obstetrics
labor, the babies died in the womb before arrival in the hospital.
For the
elective C/S done:
i. 2 were
for two previous caesarian section.
ii. 5
were cases of placenta praevis.
iii. Two
were cases of transverse lie.
These
risks factors were detected early in pregnancy and their deliveries scheduled
at term (38 weeks) of the pregnancy. The
surgeries were safe and very successful.
Other
socio-economic and cultural factors that contributed to high maternal mortality
in Bori, Ogoni.
Poverty,
ignorance, their belief system and gender inequality (especially where only the
man (the husband) can take vital decisions) were culprits causing delay in
accessing health facility early enough for appropriate care.
Some ways that religion can be
appropriately applied in the reduction of maternal mortality in Bori, Ogoni (Recommendation).
1.
Religious organizations (churches,
mosques etc.) that run maternity homes in Ogoni
should properly upgrade them with employment of well-trained and experienced
midwives, and other health workers who can effectively detect obstetric risks
in pregnancy and counsel / refer such persons to designated Hospitals for
continuation of care instead of rushing them as emergencies.
2.
Religious teachings and their
interpretations should emphasize the safety and wellbeing of mother and child
in childbirth and not so much on the mode of delivery.
3.
Religious organizations can form
pregnant women group in their churches or mosques where experienced midwives,
medical doctors and other Health workers can occasionally be invited to educate
the women on mode of delivery and their indications. So that the women would be knowledgeable and
well informed about their condition.
4.
The Hospitals should incorporate
Religious/ spiritual care into the Antenatal care program and delivery of the
pregnant woman. Formally having
chaplaincy in the hospital, where pastors/ministers of God are officially
engaged for teachings, counselling and prayers for
the pregnant women during their antenatal care, and delivery in the Hospital
will increase patronage of the Hospital and reduce maternal Mortality. These
women need prayers as they attribute most of their sickness to attacks or
manipulation from their enemies or witchcrafts, making them to seek for
prayers/help in prayers houses and mission homes.
5.
Basic Health education especially on
reproductive Health and maternal mortality should be incorporated in the
curriculum of Religious institutions/ Bible Colleges for the training of
pastors so that these pastors who are supervising this mission homes and prayer
houses can effectively collaborate with the staff at the center for the benefit
of the mothers.
6.
False "prophesies” and “visions”
should be discouraged in religious gatherings or churches.
CONCLUSION
Religion as an agent of social
development has shaped individuals and community behavior through its influence
on lifestyle motivation and world view.
Its role in healthcare utilization and improved health outcomes cannot
be overemphasized but much has to be done in the area of reproductive health
and maternal mortality in Bori, Ogoni
Conflict
of Interest: Author declared no conflict of interest
Grant: Author
did not receive any grant for the study.
REFERENCES
1.
Bill
Gate: Global Worry over Nigeria’s low rating in maternal health. Vanguard News,
www.vanguardngr.com/2018/03/global-worry-nigerias-low-rating-news,maternal-health
2.
Hogan,
Margaret C., et al. (2010) "Maternal mortality for 181 countries,
1980-2008: A systematic analysis of progress towards Millennium Development
Goal 5." The Lancet 375:
1609-1623.
..
3.
CIA World
Factbook. (2015). Nigeria
Maternal Mortality Rate. Retrieved from www. Index mundi. com/nigeria/maternal mortality
rate.html.
4.
Sloan RP.
(2009). Blind Faith: The Unholy Alliance of Religion and Medicine. New York,
NY: St. Martin's Press; 2006
\
5.
Emile Durkhem(1858-1917): Theories of Functionalism, Anomie and
Division of labourhttps://www.sociologyguide.com August 2021
6.
Malinowskis concept of culture (2021) Sociology
guide.com
7.
Udoma EJ, Asuquo
EEJ, Ekott MI. (2008). Maternal Mortality from Obstructed Labour. The Role of Spiritual Churches. Int. J. Obst. &Gynae. 1999 103-105. Nigerian Journal of Clinical Practice March.
Vol.11 (2) Reasons For Preference of Delivery.
8.
Exodus
1:15-21. (2014).The Story of the Hebrew Women. The Holy Bible King James
version Bible Society of Nigeria Lagos.
9.
Hosea
4:6,”My people perish for lack of knowledge”. The Holy Bible King James Version
Bible Society of Nigeria Lagos, 2014
10.
Ugwuandde Kok
(2015)Socio-cultural factors, gender
roles and religious ideologies contributing to Caesarian-section refusal in
Nigeria Reproductive Health volume 12,
Article number: 70.
11.
Maguranyanga B.(2011).
Apostolic Religion, Health and utilization of materials and child health
services in Zimbabwe, Research report, UNICEF Country Office, Harare, Zimbabwe.
12.
Genesis 1:28 (2014) “Go ye and multiply
and fill the earth”. The Holy Bible, King James Version. Bible society of
Nigeria Lagos.
13.
Tanyi RA. (2006). Spirituality and family
nursing: spiritual assessment and interventions for families. J Adv Nurs., 53(2):287-294.
14.
Hebrew 9:22 (2014). “Without the
shedding of blood no remission” The Holy Bible King James version Bible Society
of Nigeria Lagos.
15.
Niger Delta Liberation Project. (2005).
my story, Ken Saro-wiwa. Statement to the military
Tribunal