INTRODUCTION
Fatty
liver or hepatic steatosis is the accumulation of triglycerides in the
hepatocytes which occurs when intrahepatic fat is greater than or equal 5% of
Liver weight. (1)
Hepatitis B(HBV) is a global health challenge
which affects over 2 billion people and results in over 600,000 annual deaths. (2)
Globally, viral hepatitis B and C are leading
causes of chronic liver disease(3) though there has been a predictable
decline in recent years due to the availability of ‘cure’ for hepatitis C, and an increased global preventative
strategy for HBV. Furthermore, the availability of newer and better treatment
options, well placed control and preventative measures has resulted in a
decline in CLD- related age adjusted mortalities from 21 deaths/100,000 persons
to 16 deaths/100,000 persons from 1990-2017. (4)
Chronic hepatitis B (CHB) infection is highly
prevalent in Sub-Saharan Africa with a 5-20% carrier rate in the general
population and a high mortality of up to 10.8/100,000 in some regions.(5) Lazano et al (6) reported an increasing trend in cirrhosis
related mortality of up to 31% within a 20 year period (1990-2010) with viral
hepatitis related cirrhosis as a major etiology. Arguably, chronic viral
hepatitis related cirrhosis and Hepatocellular carcinoma could rank among the
top ten causes of mortality worldwide. (7)
In
a 2017 report from 193 countries by the global, regional and national
collaboration on the burden of cirrhosis(8), hepatitis B was reported to account
for 31.5% and 24% of cirrhosis-related deaths in men and women respectively. In
the same report, hepatic steatosis was reported as the cause of death in 7.7%
and 11.3% of men and women respectively. (8)
Patients with CHB are also affected by lifestyle
related challenges of obesity, alcoholic liver disease (ALD), Metabolic
associated liver disease (MALD) or Non-alcoholic fatty liver disease (NAFLD)
affecting the larger populace. Thus, there is a global trend towards increased
alcohol consumption (9) accounting for 30-50% of cirrhosis
related death (10,11) and a disproportionate chronic liver
disease and cirrhosis- related mortality in young people less than 45years of
age (12,13) which is the same age bracket most
affected by CHB- related liver diseases in Sub-Saharan Africa. (14)
With the increasing burden of alcohol and metabolic
fatty liver disease in Africa owing to the adoption of western lifestyle, obesity,
diabetes mellitus, HIV and much more added to the already existing high
prevalence and incidence of viral hepatitis occasioned by poor screening,
inadequate disease surveillance and poor access to healthcare, CHB- related
liver diseases especially NAFLD may soon be a major cause of morbidity and
mortality in Africa identical to that of HIV and malaria.
METHODOLOGY
Study site and Participants: This was a
cross-sectional study of 114 chronic viral hepatitis B patients attending the
Gastroenterology outpatient clinic of the Rivers State University Teaching
Hospital (RSUTH) in southern Nigeria between November 2022-April 2023. Data was
collected through review of hepatitis B register and patients’ interview.
Ethical approval was obtained from the hospital ethical committee with approval
number RSUTH/REC/2022213.
Inclusion criteria: eligible adult
patients who are 18years and above with HbeAg
positivity for > 6months who gave an informed consent were included in the
study.
Exclusion criteria: Patients <18years
of age, with a self-reported history of significant alcohol consumption >14
units/day and/or pregnant females were excluded. Also, patients who are known
diabetic, and those who are positive for HCV antibody and/or HIV were excluded
from the study.
Materials and method: All study participants were screened for baseline parameters
including HCV-Ab, HIV, Fasting blood sugar (FBS), total cholesterol (CHOL), low
density cholesterol (LDL), high density cholesterol (HDL), triglyceride (TG),
ammonium aminotransferase (ALT) and aspartate aminotransferase (AST) were
measured with enzymatic photometry on blood samples. Height and weight were
evaluated and Body mass index (BMI) was calculated with weight (in kilograms)
over height squared (in meters). Persons with BMI 18.5 to 24.9 was considered
normal Persons, with BMI of more than 25-29.99 were considered overweight, and
more than 30 obese.
Abdominal sonography was performed by an
expert radiologist to detect the presence of hepatic steatosis. Hepatic
steatosis which is fat accumulation of >5% in the hepatocytes was graded
into mild, moderate and severe (15): -
Mild Hepatic steatosis: diagnosed when there
was raised hepatic echogenicity in contrast to the kidney cortex.
Moderate Hepatic
steatosis:
in addition to raised echogenicity there is blurring of the vessels.
Severe Hepatic
steatosis:
Severe form of fatty liver was diagnosed based on disappearance of diaphragm in
addition to the features of the mild and moderate form.
Data
was analyzed using the statistical software package SPSS version 22. Bivariate
logistic regression analysis was used to identify variables influencing Hepatic
steatosis and p-values <0.05 were considered statistically significant.
RESULTS
Socio-Demography
of the Study Population
This
was a cross-sectional study of 114 chronic hepatitis B infected patients with a
mean age of 36.04 ± 7.238years (range 18-44years). (figures 1 & 2). Chronic
HBV patients with a significant history of alcohol consumption were excluded
from the study.
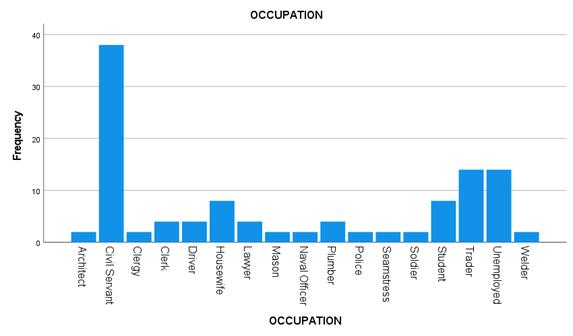
There was a predominance of males in the
study population compared to females (68, 59.6%: 46, 40.4%), and a larger
proportion of the study population were civil servants and unemployed persons
(38[33.3%], 14[12.3%]). figure 3. The study participants were fairly educated
(table 1) with a strong urban residency (112, 91.2%).
Figure 1: age distribution of the study
population.
PRESENTING
COMPLAINTS AT FIRST VISIT
There
were varied presenting complaints by the participants at their first presentation
to the clinic as shown in table 4, the most common of which was fatigue (18.2%).
Others were abdominal swelling (10.2%), early satiety (3.4%), abdominal pain
(3.4%), and leg swelling (4.5%). Notably, non-gastrointestinal related complaints
comprised a significant proportion (19.3%) of patients’ complaints at first
visit. Furthermore, 2.3% of our study population was diagnosed of hepatitis B
during compulsory pre-employment screening.
Table 4: frequency of presenting complaint of
the study population
|
Complaint Frequency Percentage
|
None 64 36.4
Early
Satiety 6 3.4
Fatigue 32
18.2
Abdominal
Pain 6 3.4
Abdominal
Swelling 18 10.2
Anorexia 4 2.3
Leg
Swelling 8 4.5
Others 34
19.3
Pre-Employment 4 2.3
DISCUSSION
This
retrospective study of 114 chronic HBV patients sought to examine the association
between Hepatic steatosis and possible risk factors in a Nigerian cohort.
Globally, studies on Hepatic steatosis,
especially on the NAFLD/MAFLD subset has gained preeminence in recent years
including studies on Hepatic steatosis in viral hepatitis B. There is however a
dearth of information on the burden and spectrum of NAFLD in African
populations, both from population-based and clinical studies (16). The paltry clinic- based studies
available are mostly in Type 2 Diabetes mellitus and HIV and the reported
prevalence of sonographically detected NAFLD in Nigeria varies from 9.5% to
68.8%.(17–20) Our reported prevalence of 29.8% is
also in consonance with these reported figures and is similar to the prevalence
trends obtained in Asia (21) and the western world. (22)
Our
observation of a higher number of males with Hepatic steatosis compared with
females (χ2 = 5.696, p = 0.017) is similar to a finding in a South
African study that reported a lower Hepatic fat content in African women. (23)
Consistent with findings from other studies (24,25),
we observed that older age( r = 0.295, p = 0.026) and hyperglycemia
(r = 0.457, p < 0.001) were significantly associated with the
incident of Hepatic steatosis. Also in accordant with other studies (26–28), our study showed that there is an
increased risk for Hepatic steatosis in patients with raised ALT levels (r =
0.292, p = 0.002). Moreover, our finding that obesity is an independent
risk factor for Hepatic steatosis in chronic HBV subjects (r = 0.553, p
< 0.001) was consistent with other studies and is similar with the general
population. (29,30)
The spectra of presenting complaints of the
patients in our study (table 4) divulge that most of our patients present late
when symptoms of Liver disease have developed. It is a well-known fact that HBV
infection is mostly asymptomatic and symptoms only develop when there is some
degree of hepatic impairment. This then underlines the exigency for a
comprehensive national screening program for viral hepatitis in countries with
high endemicity such as Nigeria.
Lastly, in our retrospective cohort, we
explored the relationship between viral parameters namely the level of HBV DNA
and HbeAg status and the presence of Hepatic
steatosis. contradictory to other studies (31,32) we observed no cogent relationship
between HBV DNA viral load and the risk of Hepatic steatosis (r = -0.088, p
= 0.354). Our study also demonstrated that the presence of steatosis correlated
positively with HbeAg (χ2 = 15.774, p
< 0.001) negativity converse to the finding by Huang et al. (33)
Study limitation: our study is limited by the
non-availability of histological data to further stage Hepatic steatosis in our
patients as well as the absence of data parameters on factors such as
dyslipidemia. Moreover, the retrospective nature of our study is also a
limitation and a well-designed prospective study will be needed to thoroughly
investigate the interplay between Hepatic steatosis and CHB.
CONCLUSION
In
our retrospective study multiple metabolic and virological factors were
significant potential determinants of Hepatic steatosis in our cohort including
male sex, older age, HbeAg positivity, raised ALT
levels, elevated BMI or obesity and hyperglycemia. Concurrent Hepatic steatosis
and CHB could potentiate the development of NASH and fibrosis in hepatitis B
infected patients.
Acknowledgments: We appreciate all
the interns and residents of gastroenterology team who painstakingly assisted
in the data collection process.
Competing interest: the authors declare
no conflict of interest.
REFERENCES
1. Nassir F, Rector RS, Hammoud GM, Ibdah JA.
Pathogenesis and Prevention of Hepatic Steatosis. Gastroenterol Hepatol. 2015
Mar;11(3):167–75.
2. Rizzetto M, Ciancio A. Chronic HBV-related
liver disease. Mol Aspects Med. 2008;29(1–2):72–84.
3. Cheemerla S, Balakrishnan M. Global
Epidemiology of Chronic Liver Disease. Clin Liver Dis. 2021 Jun 4;17(5):365–70.
4. Waheed Y, Siddiq M, Jamil Z, Najmi MH.
Hepatitis elimination by 2030: Progress and challenges. World J Gastroenterol.
2018 Nov 28;24(44):4959–61.
5. Kiire CF. The epidemiology and prophylaxis
of hepatitis B in sub-Saharan Africa: a view from tropical and subtropical
Africa. Gut. 1996;38(Suppl 2):S5-12.
6. Lozano R, Naghavi M, Foreman K, Lim S,
Shibuya K, Aboyans V, et al. Global and regional mortality from 235 causes of
death for 20 age groups in 1990 and 2010: a systematic analysis for the Global
Burden of Disease Study 2010. Lancet Lond Engl. 2012 Dec 15;380(9859):2095–128.
7. Lemoine M, Eholié S, Lacombe K. Reducing the
neglected burden of viral hepatitis in Africa: strategies for a global
approach. J Hepatol. 2015 Feb;62(2):469–76.
8. GBD 2017 Cirrhosis Collaborators. The
global, regional, and national burden of cirrhosis by cause in 195 countries
and territories, 1990-2017: a systematic analysis for the Global Burden of
Disease Study 2017. Lancet Gastroenterol Hepatol. 2020 Mar;5(3):245–66.
9. Cheemerla S, Balakrishnan M. Global
Epidemiology of Chronic Liver Disease. Clin Liver Dis. 2021 Jun 4;17(5):365–70.
10. Moon AM, Singal AG, Tapper EB. Contemporary
Epidemiology of Chronic Liver Disease and Cirrhosis. Clin Gastroenterol Hepatol
Off Clin Pract J Am Gastroenterol Assoc. 2020 Nov;18(12):2650–66.
11. Stein E, Cruz-Lemini M, Altamirano J, Ndugga
N, Couper D, Abraldes JG, et al. Heavy daily alcohol intake at the population
level predicts the weight of alcohol in cirrhosis burden worldwide. J Hepatol.
2016 Nov;65(5):998–1005.
12. Yoon Y, Chen C. Surveillance report #105liver
cirrhosis mortality in the United States: national, state and regional trends,
2000–2013. technical report, National institute of alcohol abuse and
alcoholism. Oct 2016
13. Kim D, Li AA, Gadiparthi C, Khan MA,
Cholankeril G, Glenn JS, et al. Changing Trends in Etiology-Based Annual
Mortality From Chronic Liver Disease, From 2007 Through 2016. Gastroenterology.
2018 Oct;155(4):1154-1163.e3.
14. Spearman CW, Afihene M, Ally R, Apica B, Awuku
Y, Cunha L, et al. Hepatitis B in sub-Saharan Africa: strategies to achieve the
2030 elimination targets. Lancet Gastroenterol Hepatol. 2017 Dec 1;2(12):900–9.
15. Azarkar G, Zeinali T, Sharifzadeh G, Abedi F,
Hajihosseini M, Ziaee M. Prevalence of Non-Alcoholic Fatty Liver and its
Related Factors in Birjand, During Year 2015. Mod Care J [Internet]. 2016
[cited 2023 Jun 8];13(4). Available from:
https://brieflands.com/articles/mcj-58829.html#abstract
16. Paruk IM, Pirie FJ, Motala AA. Non-alcoholic
fatty liver disease in Africa: a hidden danger. Glob Health Epidemiol Genomics.
2019 Jan;4:e3.
17. Onyekwere C, Ogbera A, Balogun B. Non-alcoholic fatty liver disease and the
metabolic syndrome in an urban hospital serving an African community. Annals of
Hepatology; 2011:10(2):119-124.
18. Olusanya T, Lesi O, Adeyomoye A, Fasanmade O. Non-alcoholic fatty liver
disease in a Nigerian population with type II diabetes mellitus. Pan African
Medical Journal. 2016;24:20. [doi: 10.11604/pamj.2016.24.20.8181]
19. Afolabi BI, Ibitoye BO, Ikem RT, Omisore AD,
Idowu BM, Soyoye DO. The Relationship Between Glycaemic Control and
Non-Alcoholic Fatty Liver Disease in Nigerian Type 2 Diabetic Patients. J Natl
Med Assoc. 2018 Jun;110(3):256–64.
20. Abere S, Orupabo B. Duration of HAART use: A
key prognosticator for NAFLD in HAART experienced HIV patients. GSC Adv Res
Rev. 2022;10(3):071–9.
21. Tong X, Song Y, Yin S, Wang J, Huang R, Wu C,
et al. Clinical impact and mechanisms of hepatitis B virus infection concurrent
with non-alcoholic fatty liver disease. Chin Med J (Engl). 2022 Jul
20;135(14):1653–63.
22. Younossi ZM, Koenig AB, Abdelatif D, Fazel Y,
Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver
disease-Meta-analytic assessment of prevalence, incidence, and outcomes.
Hepatol Baltim Md. 2016 Jul;64(1):73–84.
23. Naran NH, Haagensen M, Crowther NJ. Steatosis
in South African women: How much and why? PLoS One. 2018 Jan 19;13(1):e0191388.
doi: 10.1371/journal.pone.0191388. PMID: 29351564; PMCID: PMC5774768.
24. Zhu L, Jiang J, Zhai X, Baecker A, Peng H,
Qian J, et al. Hepatitis B virus infection and risk of non-alcoholic fatty
liver disease: A population-based cohort study. Liver Int Off J Int Assoc Study
Liver. 2019 Jan;39(1):70–80.
25. Younossi ZM, Koenig AB, Abdelatif D, Fazel Y,
Henry L, Wymer M. Global epidemiology of nonalcoholic fatty liver
disease-Meta-analytic assessment of prevalence, incidence, and outcomes.
Hepatol Baltim Md. 2016 Jul;64(1):73–84.
26. Sanyal D, Mukherjee P, Raychaudhuri M, Ghosh
S, Mukherjee S, Chowdhury S. Profile of liver enzymes in non-alcoholic fatty
liver disease in patients with impaired glucose tolerance and newly detected
untreated type 2 diabetes. Indian J Endocrinol Metab. 2015;19(5):597–601.
27. Hadizadeh F, Faghihimani E, Adibi P.
Nonalcoholic fatty liver disease: Diagnostic biomarkers. World J Gastrointest
Pathophysiol. 2017 May 15;8(2):11–26.
28. Kim SU, Jeon MY, Lim TS. Diagnostic
Performance of Serum Asialo-α1-acid Glycoprotein for Advanced Liver
Fibrosis or Cirrhosis in Patients with Chronic Hepatitis B or Nonalcoholic
Fatty Liver Disease. Korean J Gastroenterol Taehan Sohwagi Hakhoe Chi. 2019 Dec
25;74(6):341–8.
29. Charatcharoenwitthaya P, Pongpaibul A,
Kaosombatwattana U, Bhanthumkomol P, Bandidniyamanon W, Pausawasdi N, et al.
The prevalence of steatohepatitis in chronic hepatitis B patients and its
impact on disease severity and treatment response. Liver Int Off J Int Assoc
Study Liver. 2017 Apr;37(4):542–51.
30. Lee JY, Kim KM, Lee SG, Yu E, Lim YS, Lee HC,
et al. Prevalence and risk factors of non-alcoholic fatty liver disease in
potential living liver donors in Korea: a review of 589 consecutive liver
biopsies in a single center. J Hepatol. 2007 Aug;47(2):239–44.
31. Wang MM, Wang GS, Shen F, Chen GY, Pan Q, Fan
JG. Hepatic steatosis is highly prevalent in hepatitis B patients and negatively
associated with virological factors. Dig Dis Sci. 2014 Oct;59(10):2571–9.
32. Hui RWH, Seto WK, Cheung KS, Mak LY, Liu KSH,
Fung J, et al. Inverse relationship between hepatic steatosis and hepatitis B
viremia: Results of a large case-control study. J Viral Hepat. 2018
Jan;25(1):97–104.
33. Huang Y, Gan Q, Lai R, Wang W, Guo S, Sheng Z,
et al. Application of Fatty Liver Inhibition of Progression Algorithm and
Steatosis, Activity, and Fibrosis Score to Assess the Impact of Non-Alcoholic
Fatty Liver on Untreated Chronic Hepatitis B Patients. Front Cell Infect
Microbiol. 2022 Jan 17;11:733348.