Millard-Gubler syndrome (MGS) is a brainstem syndrome
characterized by ipsilateral sixth and seventh cranial nerve palsies and
contralateral hemiparesis. Pontine stroke is the commonest cause of MGS even
though other non-vascular etiologies have been
described in the literature. MGS resulting from pontine infarction is
associated with relatively good prognosis, even though the overall prognosis
is influenced by other factors.
We report a case
of 52-year-old hypertensive with both clinical and imaging evidence of
Millard -Gubler syndrome with cerebellar ataxia
following a pontinehemorrhage.
He managed conservatively and was discharged after about three weeks on
admission. He has remained clinically stable since after discharge.
Millard -Gubler
Syndrome (MGS) is a rare type of brainstem syndrome specifically involving
ventral pontine area, affecting the 6th and 7th cranial
nerves as well as the corticospinal tracts and was first described in 1958(1). The
core features of MGS consist of ipsilateral lateral rectus palsy,
ipsilateral facial palsy, and contralateral hemiparesis of the upper and lower
limbs. Generally, stroke is the common cause of this syndrome, even though
other non-vascular etiologies have been
profusely documented in the literature (1–3)
Brainstem stroke is the most lethal form
of all strokes, and globally contributes significantly to a significant cause
of mortality and morbidity(4,5).
Although ischemic accounts for the majority of the vascular events in the brain
stem, pons appear to be the commonest site of spontaneous brainstem hemorrhage (6).
Spontaneous brainstem hemorrhage constitutes about 1/10th of all
intracerebral hemorrhages with an annual incidence of roughly 2-4/100,000 per
year (6–8) and
pons is most common site of bleed (60-80%)(4,9) and
individuals in their 4th and 5th decades are mostly
involved with more males affected. Vascular lesion to the brain stem disrupts a
plethora of physiological functions such as respiration, cardiac rhythm, blood
pressure control, consciousness, and the sleep-wake cycle.
We report a case of a middle-aged man,
known hypertensive, who presented to us with clinical features of Millard Gubler syndrome following anterior pontine hemorrhage and
was conservatively managed successfully.
CASE REPORT
We presented a 52-year-old male state security operative
and a known hypertensive who was admitted into our facility with a new onset acute
right upper and lower limb weakness with associated left-sided gaze impairment
and facial palsy. There was a preceding history of generalized, severe, and
throbbing headache, which was transiently responsive to analgesics. He also had
accompanying episodes of projectile vomiting, which later resolved
spontaneously. Apart from dysarthria, he did not experience dizziness or
dysphagia and consciousness was preserved.
Patient had
significantly used marijuana and tobacco for more than 5 years up until the
time of his sickness. He, however, took alcoholic beverages occasionally.
However, he denied history of intravenous drug use.
Apart from
hypertension, he did not volunteer a history of type 2 diabetes and random
blood sugar tested on admission was normal. On further questioning, he
disclosed poor adherence to his antihypertensives
medications despite enrolling into a health insurance program. He had never
experienced a transient ischemic attack in the past. Family history of
hypertension or type diabetes mellitus could not be ascertained. Patient was
married in a monogamous family with three (3) adult children (2 females and a
male).
At presentation, he
was fully conscious, but restless and diaphoretic and had severely elevated
blood pressure (250/170 mmHg) with displaced heaving apex. Oxygen saturation
was 95% at the room air. Other significant findings noted were left abducens and facial nerve palsies with intact left
adduction and preserved upward gaze. The contralateral cranial nerves were
intact (see Table 1 below). However, there was weakness (power grade 4/5) of
the contralateral upper and lower limbs. In addition, he had left appendicular
cerebellar signs such as ataxia and dysmetria. Other
systems were essentially intact.
His investigation
results, including serology tests for HIV, Hepatitis B virus and Hepatitis C
Virus, were all negative; urinalysis revealed moderate proteinuria (2+); full
blood count parameters equally showed normal findings; both initial and repeat
serum electrolyte urea and creatine results showed
normal parameters as shown in Table 1. His Electrocardiogram (ECG) result
showed inferior lateral ischemic infarcts, left ventricular hypertrophy with
strain pattern, reciprocal changes, and left axis deviation (LAD).
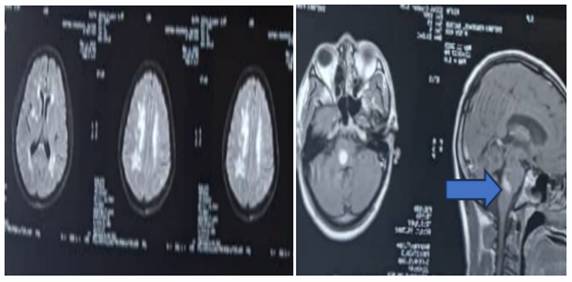
Brain magnetic
resonance imaging (MRI) showed pontine hemorrhage with background white matter
microvascular infarcts as shown in Figure 2
Patient was managed
conservatively in accordance with the recommended guidelines for managing
hemorrhagic stroke, including management of hypertension, intracranial
pressure, and comorbidities. He received oral antihypertensive drugs, 20%
intravenous mannitol and multivitamins. Neurorehabilitation
was also activated.
His clinical state
improved significantly within two weeks of hospitalization and was discharged a
week later to the Neurology Outpatient Clinic for follow up. The patient has remained
stable since after discharge and his visual symptoms have also improved
remarkably.
Millard-Gubler
syndrome is a rare brainstem disorderresulting from a lesion to the ventral pons (1).
The classical features of this syndrome comprise ipsilateral facial nerve
palsy, ipsilateral abducens palsy and contralateral hemiplegia (1,10). Millard-Gubler syndrome (MGS) is an
eponym after two French physicians, Auguste Louis
Jules Millard and Adolphe-Marie Gubler
who first described the features of this syndrome in 1858.The
first description of this condition was in association with a pontine mass (1,2).
Since then, other etiologies have been described with stroke accounting for
most of the cases of MGS ((11–14) )
Our patient presented with all the classical features MGS in addition to the
left limb ataxia and dysmetria. Cerebellar features can sometimes be associated
with this syndrome depending on the extent of the lesion, Interruption of the
cerebellopontine fibres is though to be responsible for the emergence of these
features in MGS (15).
Another case of MGS with cerebellar features was reportedby Ayele et al in Ethiopia in a 55-year- old
male that suffered a pontine infarction.(15) .
It was curious this patient did not have hypertension as well as other
traditional cardiovacular risks, even though he was not extensively
investigated for other rare causes of ischemic stroke such as monogenic
arteriopathies.However, for our
patient, there was a lon standing history of hypertension (16).
Compared to brainstemhemorrhage,pontine infarction appears to have been more frequently described in
various case reports of MGS than the former. For both ischemic and haemorrhagic
strokes, uncontrolled hypertension is the main driver of these events, and poor
adherence to to the prescribed treatments remains a major cause. Our patient
admitted to a history of poor drug compliance and that reflected in his high
admission blood pressure. As mentioned above, hypertension remains the most
important risk factor of stroke, irrespective of the subtype (16,17), and measures to address stroke risks should be part of the strategies
towards steming stroke tide. These measures should be incorporated into stroke
education for patients.
Our
patient was a middle-aged man in his 50’s and in this age bracket, the
commonest cause of Millard-Gubler syndrome (MGS) is
vascular, whether haemorrhagic or ischemic stroke (5). In terms of the vascular territory involved, occlusion
or rupture of the short circumferential branch of the basilar artery formed by
the confluence of the vertebral arteries could be the reason for the emergence
of symptoms of MGS (4). Sometimes, compression of pontine arteries by subarachnoid
haemorrhage or a space-occupying lesion can also lead
to MGS, (8,18) Rarely, a brain stem cavernous vascular
malformation may cause MGS, especially if a recent bleed has happened (3,8) . For our patient, although it was clear that
uncontrolled hypertension caused his brainstem bleed, the specific vessels
involved could not be ascertained since an angiography of the brain was not
conducted. In the younger age group, common causes of MGS include tumours, infections (e.g., neurocysticercosis),(13) viral infection (e.g., rhombencephalitis),
demyelinating disease (e.g., multiple sclerosis), and immune-mediated
inflammatory disorders, such as neuro-Behçet's
disease (11).
Primary brainstem hemorrhage
is usually associated with the worst prognosis of all types of brainstem ICH,
and prognosis will depend on factors such as age, presence of coma, blood
glucose, Glasgow Coma Scale (GCS), hemorrhage size, location, and extent of
hemorrhage (6,8). Our
patient had some of these variables in his favor, especially the fact he never
lost consciousness right from the admission, and his blood sugar level was also
within normal limit. These factors as well as other possible covert variables
might have influenced his excellent clinical outcome despite suffering a
potential life-threatening condition.
Finally, our patient made a significant
clinical improvement within three weeks of (6)hospitalization and was
successfully discharged. Good clinical out have also been documented following
brainstem stroke in other case reports. (9,10).
CONCLUSION
This case report has
achieved two important purposes. Firstly, it has provided an opportunity to
showcase a rare ventral pontine syndrome in a Nigerian patient who suffered a
pontine bled and was successfully managed. It has also reechoed the strategic
role of brain imaging, especially magnetic resonance imaging, in confirming
diagnosis and differentiating it from other differential diagnoses. Complete
recovery is usually expected with supportive treatment and in the absence of
any major complications.
Cite this Article:Nwazor E, Martyns-Yellow
T, Chikeka C, Ogbamgba S
(2024). Pontine
Haemorrhage presenting with Millard-Gubler Syndrome with Cerebellar ataxia in a 52-year-old
male Nigerian hypertensive, Nigeria. Greener Journal of Medical Sciences, 14(2): 60-64.